Hodgkin Lymphoma Treatment (PDQ®): Treatment - Health Professional Information [NCI]
General Information About Hodgkin Lymphoma (HL)
Incidence and Mortality
Estimated new cases and deaths from HL in the United States in 2024:[
- New cases: 8,570.
- Deaths: 910.
Up to 90% of all newly diagnosed patients with HL can be cured with combination chemotherapy and/or radiation therapy.[
Anatomy

The lymph system is part of the body's immune system and is made up of tissues and organs that help protect the body from infection and disease. These include the tonsils, adenoids (not shown), thymus, spleen, bone marrow, lymph vessels, and lymph nodes. Lymph tissue is also found in many other parts of the body, including the small intestine.
HL most frequently presents in lymph node groups above the diaphragm and/or in mediastinal lymph nodes. Involvement of Waldeyer's ring or tonsillar lymph glands is rarely seen.
Risk Factors
Risk factors for HL include the following:
- Being in early adulthood (aged 20–39 years) (most often) or late adulthood (aged 65 years and older) (less often).
- Being male.
- Having a previous infection with the Epstein-Barr virus in the teenage years or early childhood.
- Having a first-degree relative with HL.
Clinical Features
These and other signs and symptoms may be caused by HL or by other conditions:
- Painless, swollen lymph nodes in the neck, axilla, or inguinal area.
- Fever defined as 38ºC or higher.
- Drenching and recurrent night sweats.
- Weight loss of 10% or more of baseline weight in the previous 6 months.
- Pruritus, especially after bathing or after ingesting alcohol.
- Fatigue.
Treatment of HL should relieve these symptoms within days. For more information, see Hot Flashes and Night Sweats, Pruritus, and Fatigue.
Diagnostic Evaluation
Diagnostic evaluation of patients with lymphoma may include the following:
- Biopsy (preferably excisional), with interpretation by a qualified pathologist.
- History, with special attention given to the presence and duration of fever, night sweats, and unexplained weight loss of 10% or more of body weight in the previous 6 months.
- Physical examination.
- Laboratory tests.
- Complete blood cell count and platelet count.
- Erythrocyte sedimentation rate.
- Chemistry panel (electrolytes, blood urea nitrogen, creatinine, calcium, aspartate transaminase, alanine aminotransferase, bilirubin, and alkaline phosphatase) plus lactate dehydrogenase, uric acid, and phosphorus.
- Radiographic examination.
- Computed tomography (CT) of the neck, chest, abdomen, and pelvis; or metabolic imaging (fluorine F 18-fludeoxyglucose positron emission tomography [PET]) with PET-CT. PET-magnetic resonance imaging scans may be equivalent to PET-CT in obtaining staging information at 25% of the radiation dose.[
3 ]
- Computed tomography (CT) of the neck, chest, abdomen, and pelvis; or metabolic imaging (fluorine F 18-fludeoxyglucose positron emission tomography [PET]) with PET-CT. PET-magnetic resonance imaging scans may be equivalent to PET-CT in obtaining staging information at 25% of the radiation dose.[
- HIV testing.
- Hepatitis B and hepatitis C serology.
All stages of HL can be subclassified into A and B categories: B for those with defined general symptoms (described below) and A for those without B symptoms. The B designation is given to patients with any of the following symptoms:
- Unexplained weight loss (more than 10% of body weight in the 6 months before diagnosis).
- Unexplained fever with temperatures above 38°C.
- Drenching and recurrent night sweats.
The most significant B symptoms are fevers and weight loss. Night sweats alone do not confer an adverse prognosis.
Prognostic Factors
The prognosis for a given patient depends on several factors. The most important factors are the following:[
- Presence or absence of systemic B symptoms.
- Stage of disease.
- Presence of large masses.
- Quality and suitability of the treatment administered.
Other important factors are:[
- Age.
- Sex.
- Erythrocyte sedimentation rate.
- Hematocrit.
- Extent of abdominal involvement.
- Absolute number of nodal sites of involvement.
The best predictor of treatment failure is a PET-CT scan obtained after two cycles of chemotherapy (PET2 scan).[
Follow-Up
Recommendations for posttreatment follow-up are not evidence based, but a variety of opinions have been published for high-risk patients who present with advanced-stage disease and for patients who achieve less-than-complete remission by PET-CT scans at the end of therapy.[
For patients with negative findings from a PET-CT scan at the end of therapy, routine scans are not advised because of the very low risk of recurrence.[
Among 6,840 patients enrolled in German Hodgkin Study Group (GHSG) trials, with a median follow-up of 10.3 years, 141 patients had a relapse after 5 years, compared with 466 patients who had a relapse within 5 years. Treatment-related adverse effects and late relapses may occur beyond 20 years of follow-up.[
Adverse Long-Term Effects of Therapy
Patients who complete therapy for HL are at risk of developing long-term side effects, ranging from direct damage to organ function or the immune system to second malignancies. For the first 15 years after treatment, HL is the main cause of death. By 15 to 20 years after therapy, the cumulative mortality from a second malignancy, cardiovascular disease, or pulmonary fibrosis exceeds the cumulative mortality from HL.[
Compared with the general population, long-term survivors of HL have a significantly lower life expectancy.[
Second malignancies
Recommendations for screening for secondary malignancies or follow-up of long-term survivors are consensus based and not derived from randomized trials.[
Solid tumors
An increase in second solid tumors has also been observed, especially mesothelioma and cancers of the lung, breast, thyroid, bone/soft tissue, stomach, esophagus, colon and rectum, uterine cervix, and head and neck.[
- At 15-years of follow-up, the risk is approximately 13%.[
30 ] - At 20-years of follow-up, the risk is approximately 17%.[
35 ] - At 25-years of follow-up, the risk is approximately 22%.[
27 ,36 ] - At 40-years of follow-up, the risk is approximately 48%.[
37 ]
In a cohort of 18,862 5-year survivors from 13 population-based registries, the younger patients had elevated risks for breast, colon, and rectal cancers for 10 to 25 years before the ages when routine screening is recommended in the general population.[
Lung cancer and breast cancer are among the most-common second solid tumors that develop after therapy for HL.
- Lung cancer. Lung cancer is seen with increased frequency, even after chemotherapy alone, and the risk of this cancer increases with cigarette smoking.[
38 ,39 ,40 ,41 ] In a retrospective Surveillance, Epidemiology, and End Results (SEER) Program analysis, stage-specific survival was decreased by 30% to 60% in HL survivors, compared with patients with de novo non-small cell lung cancer.[42 ] - Breast cancer. Breast cancer is seen with increased frequency after radiation therapy or combined-modality therapy.[
27 ,28 ,43 ,44 ,45 ] The risk appears greatest for females treated with radiation before age 30 years, especially for girls close to menarche.[46 ] The incidence of breast cancer increases substantially after 15 years of posttherapy follow-up.[27 ,47 ,48 ]In two case-control studies of 479 patients who developed breast cancer after therapy for HL, cumulative absolute risks for developing breast cancer were calculated as a function of radiation therapy dose and the use of chemotherapy.[
49 ,50 ] With a 30-year to 40-year follow-up, cumulative absolute risks of breast cancer with exposure to radiation range from 8.5% to 39.6%, depending on age at diagnosis. These cohort studies show a continued increase in cumulative excess risk of breast cancer beyond 20 years of follow-up.[49 ,50 ]In a nested case-control study and subsequent cohort study, patients who received both chemotherapy and radiation therapy had a statistically significant lower risk of developing breast cancer than did those treated with radiation therapy alone.[
43 ,51 ] Reaching early menopause with fewer than 10 years of intact ovarian function appeared to account for the reduction in risk among patients who received combined-modality therapy.[51 ] Reduction of radiation volume also decreased the risk of breast cancer after HL.[51 ]
Late effects of autologous stem cell transplant for failure of induction chemotherapy include second malignancies, hypothyroidism, hypogonadism, herpes zoster, depression, and cardiac disease.[
Hematologic cancers
- Acute myelogenous leukemia (AML). Acute nonlymphocytic leukemia may occur in patients treated with combined-modality therapy or with combination chemotherapy alone, especially with increased exposure to alkylating agents.[
30 ,53 ]- At 10 years after therapy with regimens containing MOPP (mechlorethamine, vincristine, procarbazine, and prednisone), the risk of AML is approximately 3%, with the peak incidence occurring 5 to 9 years after therapy.[
30 ,53 ] The risk of acute leukemia at 10 years after therapy with ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) appears to be less than 1%.[54 ] - A population-based study of more than 35,000 survivors during a 30-year time span identified 217 patients who developed AML. The excess absolute risk (EAR) was significantly higher for older patients (>35 years at diagnosis) than for younger survivors (EAR, 9.9 vs. 4.2 per 10,000 patient-years, P < .001).[
55 ]
- At 10 years after therapy with regimens containing MOPP (mechlorethamine, vincristine, procarbazine, and prednisone), the risk of AML is approximately 3%, with the peak incidence occurring 5 to 9 years after therapy.[
Other adverse long-term effects
Treatment of HL also affects the endocrine, cardiac, pulmonary, skeletal, and immune systems. Chronic fatigue can be a debilitating symptom for some long-term survivors.[
Infertility. A toxic effect that is primarily related to chemotherapy is infertility, usually after regimens containing MOPP or BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone).[
Hypothyroidism. Hypothyroidism is a late complication primarily related to radiation therapy.[
Cardiac disease. A late complication primarily related to radiation therapy is cardiac disease, the risk of which may persist for over 30 years after the first treatment.[
In the U.K. RAPID trial, performed between 2003 and 2010, 183 patients with early-stage HL were PET-negative but still received involved-field radiation therapy (IFRT) (20 Gy) after receiving ABVD.[
Pulmonary impairment. Impairment of pulmonary function may occur as a result of mantle-field radiation therapy; this impairment is not usually clinically evident, and recovery in pulmonary testing often occurs after 2 to 3 years.[
Bone necrosis. Avascular necrosis of bone has been observed in patients treated with chemotherapy and is most likely related to corticosteroid therapy.[
Bacterial sepsis. Bacterial sepsis may occur rarely after splenectomy performed during staging laparotomy for HL;[
Fatigue. Fatigue is a commonly reported symptom among patients who have completed chemotherapy and radiation therapy. In a case-control study design, most HL survivors reported significant fatigue lasting for more than 6 months after therapy, compared with age-matched controls. Quality-of-life questionnaires given to 5,306 patients on GHSG trials showed that 20% of patients complained of severe fatigue 5 years after therapy, and those patients had significantly increased problems with employment and financial stability.[
Neurocognitive impairment. After a median of 23 years from diagnosis, 1,760 HL survivors treated in childhood were compared with 3,180 siblings. Significantly higher rates of memory loss (8.1% vs. 5.7%; P < .05), anxiety (7.0% vs. 5.4%; P < .05), unemployment (9.6% vs. 4.4%; P < .05), depression (9.1% vs. 7.0%; P < .05), and impaired physical quality of life (11.2% vs. 3.0%; P < .05) were reported.[
References:
- American Cancer Society: Cancer Facts and Figures 2024. American Cancer Society, 2024.
Available online . Last accessed June 21, 2024. - Brice P, de Kerviler E, Friedberg JW: Classical Hodgkin lymphoma. Lancet 398 (10310): 1518-1527, 2021.
- Picardi M, Cavaliere C, Della Pepa R, et al.: PET/MRI for staging patients with Hodgkin lymphoma: equivalent results with PET/CT in a prospective trial. Ann Hematol 100 (6): 1525-1535, 2021.
- Cosset JM, Henry-Amar M, Meerwaldt JH, et al.: The EORTC trials for limited stage Hodgkin's disease. The EORTC Lymphoma Cooperative Group. Eur J Cancer 28A (11): 1847-50, 1992.
- Evens AM, Helenowski I, Ramsdale E, et al.: A retrospective multicenter analysis of elderly Hodgkin lymphoma: outcomes and prognostic factors in the modern era. Blood 119 (3): 692-5, 2012.
- Agostinelli C, Gallamini A, Stracqualursi L, et al.: The combined role of biomarkers and interim PET scan in prediction of treatment outcome in classical Hodgkin's lymphoma: a retrospective, European, multicentre cohort study. Lancet Haematol 3 (10): e467-e479, 2016.
- Gallamini A, Rossi A, Patti C, et al.: Interim PET-adapted chemotherapy in advanced Hodgkin lymphoma: results of the second interim analysis of the Italian GITIL/FIL DH0607 trial. [Abstract] Hematol Oncol 33 (Suppl 1): A-118, 100-180, 2015.
- Spina V, Bruscaggin A, Cuccaro A, et al.: Circulating tumor DNA reveals genetics, clonal evolution, and residual disease in classical Hodgkin lymphoma. Blood 131 (22): 2413-2425, 2018.
- Cottereau AS, Versari A, Loft A, et al.: Prognostic value of baseline metabolic tumor volume in early-stage Hodgkin lymphoma in the standard arm of the H10 trial. Blood 131 (13): 1456-1463, 2018.
- Akhtari M, Milgrom SA, Pinnix CC, et al.: Reclassifying patients with early-stage Hodgkin lymphoma based on functional radiographic markers at presentation. Blood 131 (1): 84-94, 2018.
- Moskowitz AJ, Schöder H, Gavane S, et al.: Prognostic significance of baseline metabolic tumor volume in relapsed and refractory Hodgkin lymphoma. Blood 130 (20): 2196-2203, 2017.
- Hoppe RT, Advani RH, Ai WZ, et al.: Hodgkin lymphoma, version 2.2012 featured updates to the NCCN guidelines. J Natl Compr Canc Netw 10 (5): 589-97, 2012.
- Ng A, Constine LS, Advani R, et al.: ACR Appropriateness Criteria: follow-up of Hodgkin's lymphoma. Curr Probl Cancer 34 (3): 211-27, 2010 May-Jun.
- Armitage JO: Who benefits from surveillance imaging? J Clin Oncol 30 (21): 2579-80, 2012.
- Picardi M, Pugliese N, Cirillo M, et al.: Advanced-stage Hodgkin lymphoma: US/chest radiography for detection of relapse in patients in first complete remission--a randomized trial of routine surveillance imaging procedures. Radiology 272 (1): 262-74, 2014.
- El-Galaly TC, Mylam KJ, Brown P, et al.: Positron emission tomography/computed tomography surveillance in patients with Hodgkin lymphoma in first remission has a low positive predictive value and high costs. Haematologica 97 (6): 931-6, 2012.
- Hartridge-Lambert SK, Schöder H, Lim RC, et al.: ABVD alone and a PET scan complete remission negates the need for radiologic surveillance in early-stage, nonbulky Hodgkin lymphoma. Cancer 119 (6): 1203-9, 2013.
- Hapgood G, Zheng Y, Sehn LH, et al.: Evaluation of the Risk of Relapse in Classical Hodgkin Lymphoma at Event-Free Survival Time Points and Survival Comparison With the General Population in British Columbia. J Clin Oncol 34 (21): 2493-500, 2016.
- Bröckelmann PJ, Goergen H, Kohnhorst C, et al.: Late Relapse of Classical Hodgkin Lymphoma: An Analysis of the German Hodgkin Study Group HD7 to HD12 Trials. J Clin Oncol 35 (13): 1444-1450, 2017.
- Mauch PM, Kalish LA, Marcus KC, et al.: Long-Term Survival in Hodgkin's Disease Cancer J Sci Am 1 (1): 33-42, 1995.
- Aisenberg AC: Problems in Hodgkin's disease management. Blood 93 (3): 761-79, 1999.
- Longo DL, Armitage JO: Controversies in the treatment of early-stage Hodgkin's lymphoma. N Engl J Med 372 (17): 1667-9, 2015.
- Aleman BM, van den Belt-Dusebout AW, Klokman WJ, et al.: Long-term cause-specific mortality of patients treated for Hodgkin's disease. J Clin Oncol 21 (18): 3431-9, 2003.
- Sud A, Thomsen H, Sundquist K, et al.: Risk of Second Cancer in Hodgkin Lymphoma Survivors and Influence of Family History. J Clin Oncol 35 (14): 1584-1590, 2017.
- de Vries S, Schaapveld M, Janus CPM, et al.: Long-Term Cause-Specific Mortality in Hodgkin Lymphoma Patients. J Natl Cancer Inst 113 (6): 760-769, 2021.
- Ng AK: Current survivorship recommendations for patients with Hodgkin lymphoma: focus on late effects. Blood 124 (23): 3373-9, 2014.
- Dores GM, Metayer C, Curtis RE, et al.: Second malignant neoplasms among long-term survivors of Hodgkin's disease: a population-based evaluation over 25 years. J Clin Oncol 20 (16): 3484-94, 2002.
- Franklin J, Pluetschow A, Paus M, et al.: Second malignancy risk associated with treatment of Hodgkin's lymphoma: meta-analysis of the randomised trials. Ann Oncol 17 (12): 1749-60, 2006.
- Hodgson DC, Gilbert ES, Dores GM, et al.: Long-term solid cancer risk among 5-year survivors of Hodgkin's lymphoma. J Clin Oncol 25 (12): 1489-97, 2007.
- Swerdlow AJ, Higgins CD, Smith P, et al.: Second cancer risk after chemotherapy for Hodgkin's lymphoma: a collaborative British cohort study. J Clin Oncol 29 (31): 4096-104, 2011.
- Chowdhry AK, McHugh C, Fung C, et al.: Second primary head and neck cancer after Hodgkin lymphoma: a population-based study of 44,879 survivors of Hodgkin lymphoma. Cancer 121 (9): 1436-45, 2015.
- Dores GM, Curtis RE, van Leeuwen FE, et al.: Pancreatic cancer risk after treatment of Hodgkin lymphoma. Ann Oncol 25 (10): 2073-9, 2014.
- Rigter LS, Spaander MCW, Aleman BMP, et al.: High prevalence of advanced colorectal neoplasia and serrated polyposis syndrome in Hodgkin lymphoma survivors. Cancer 125 (6): 990-999, 2019.
- Geurts YM, Shakir R, Ntentas G, et al.: Association of Radiation and Procarbazine Dose With Risk of Colorectal Cancer Among Survivors of Hodgkin Lymphoma. JAMA Oncol 9 (4): 481-489, 2023.
- O'Brien MM, Donaldson SS, Balise RR, et al.: Second malignant neoplasms in survivors of pediatric Hodgkin's lymphoma treated with low-dose radiation and chemotherapy. J Clin Oncol 28 (7): 1232-9, 2010.
- Bonadonna G, Viviani S, Bonfante V, et al.: Survival in Hodgkin's disease patients--report of 25 years of experience at the Milan Cancer Institute. Eur J Cancer 41 (7): 998-1006, 2005.
- Schaapveld M, Aleman BM, van Eggermond AM, et al.: Second Cancer Risk Up to 40 Years after Treatment for Hodgkin's Lymphoma. N Engl J Med 373 (26): 2499-511, 2015.
- van Leeuwen FE, Klokman WJ, Stovall M, et al.: Roles of radiotherapy and smoking in lung cancer following Hodgkin's disease. J Natl Cancer Inst 87 (20): 1530-7, 1995.
- Swerdlow AJ, Schoemaker MJ, Allerton R, et al.: Lung cancer after Hodgkin's disease: a nested case-control study of the relation to treatment. J Clin Oncol 19 (6): 1610-8, 2001.
- Travis LB, Gospodarowicz M, Curtis RE, et al.: Lung cancer following chemotherapy and radiotherapy for Hodgkin's disease. J Natl Cancer Inst 94 (3): 182-92, 2002.
- Lorigan P, Radford J, Howell A, et al.: Lung cancer after treatment for Hodgkin's lymphoma: a systematic review. Lancet Oncol 6 (10): 773-9, 2005.
- Milano MT, Li H, Constine LS, et al.: Survival after second primary lung cancer: a population-based study of 187 Hodgkin lymphoma patients. Cancer 117 (24): 5538-47, 2011.
- van Leeuwen FE, Klokman WJ, Stovall M, et al.: Roles of radiation dose, chemotherapy, and hormonal factors in breast cancer following Hodgkin's disease. J Natl Cancer Inst 95 (13): 971-80, 2003.
- Wahner-Roedler DL, Nelson DF, Croghan IT, et al.: Risk of breast cancer and breast cancer characteristics in women treated with supradiaphragmatic radiation for Hodgkin lymphoma: Mayo Clinic experience. Mayo Clin Proc 78 (6): 708-15, 2003.
- Travis LB, Hill DA, Dores GM, et al.: Breast cancer following radiotherapy and chemotherapy among young women with Hodgkin disease. JAMA 290 (4): 465-75, 2003.
- Moskowitz CS, Ronckers CM, Chou JF, et al.: Development and Validation of a Breast Cancer Risk Prediction Model for Childhood Cancer Survivors Treated With Chest Radiation: A Report From the Childhood Cancer Survivor Study and the Dutch Hodgkin Late Effects and LATER Cohorts. J Clin Oncol 39 (27): 3012-3021, 2021.
- Alm El-Din MA, Hughes KS, Finkelstein DM, et al.: Breast cancer after treatment of Hodgkin's lymphoma: risk factors that really matter. Int J Radiat Oncol Biol Phys 73 (1): 69-74, 2009.
- Cooke R, Jones ME, Cunningham D, et al.: Breast cancer risk following Hodgkin lymphoma radiotherapy in relation to menstrual and reproductive factors. Br J Cancer 108 (11): 2399-406, 2013.
- Travis LB, Hill D, Dores GM, et al.: Cumulative absolute breast cancer risk for young women treated for Hodgkin lymphoma. J Natl Cancer Inst 97 (19): 1428-37, 2005.
- Swerdlow AJ, Cooke R, Bates A, et al.: Breast cancer risk after supradiaphragmatic radiotherapy for Hodgkin's lymphoma in England and Wales: a National Cohort Study. J Clin Oncol 30 (22): 2745-52, 2012.
- De Bruin ML, Sparidans J, van't Veer MB, et al.: Breast cancer risk in female survivors of Hodgkin's lymphoma: lower risk after smaller radiation volumes. J Clin Oncol 27 (26): 4239-46, 2009.
- Lavoie JC, Connors JM, Phillips GL, et al.: High-dose chemotherapy and autologous stem cell transplantation for primary refractory or relapsed Hodgkin lymphoma: long-term outcome in the first 100 patients treated in Vancouver. Blood 106 (4): 1473-8, 2005.
- Koontz MZ, Horning SJ, Balise R, et al.: Risk of therapy-related secondary leukemia in Hodgkin lymphoma: the Stanford University experience over three generations of clinical trials. J Clin Oncol 31 (5): 592-8, 2013.
- Valagussa P, Santoro A, Fossati-Bellani F, et al.: Second acute leukemia and other malignancies following treatment for Hodgkin's disease. J Clin Oncol 4 (6): 830-7, 1986.
- Schonfeld SJ, Gilbert ES, Dores GM, et al.: Acute myeloid leukemia following Hodgkin lymphoma: a population-based study of 35,511 patients. J Natl Cancer Inst 98 (3): 215-8, 2006.
- Kreissl S, Müller H, Goergen H, et al.: Health-Related Quality of Life in Patients With Hodgkin Lymphoma: A Longitudinal Analysis of the German Hodgkin Study Group. J Clin Oncol 38 (25): 2839-2848, 2020.
- Dores GM, Curtis RE, Dalal NH, et al.: Cause-Specific Mortality Following Initial Chemotherapy in a Population-Based Cohort of Patients With Classical Hodgkin Lymphoma, 2000-2016. J Clin Oncol 38 (35): 4149-4162, 2020.
- Behringer K, Breuer K, Reineke T, et al.: Secondary amenorrhea after Hodgkin's lymphoma is influenced by age at treatment, stage of disease, chemotherapy regimen, and the use of oral contraceptives during therapy: a report from the German Hodgkin's Lymphoma Study Group. J Clin Oncol 23 (30): 7555-64, 2005.
- van der Kaaij MA, Heutte N, Le Stang N, et al.: Gonadal function in males after chemotherapy for early-stage Hodgkin's lymphoma treated in four subsequent trials by the European Organisation for Research and Treatment of Cancer: EORTC Lymphoma Group and the Groupe d'Etude des Lymphomes de l'Adulte. J Clin Oncol 25 (19): 2825-32, 2007.
- Scholz M, Engert A, Franklin J, et al.: Impact of first- and second-line treatment for Hodgkin's lymphoma on the incidence of AML/MDS and NHL--experience of the German Hodgkin's Lymphoma Study Group analyzed by a parametric model of carcinogenesis. Ann Oncol 22 (3): 681-8, 2011.
- Behringer K, Mueller H, Goergen H, et al.: Gonadal function and fertility in survivors after Hodgkin lymphoma treatment within the German Hodgkin Study Group HD13 to HD15 trials. J Clin Oncol 31 (2): 231-9, 2013.
- Viviani S, Santoro A, Ragni G, et al.: Pre- and post-treatment testicular dysfunction in Hodgkin's disease (HD). [Abstract] Proceedings of the American Society of Clinical Oncology 7: A-877, 227, 1988.
- van der Kaaij MA, Heutte N, Meijnders P, et al.: Premature ovarian failure and fertility in long-term survivors of Hodgkin's lymphoma: a European Organisation for Research and Treatment of Cancer Lymphoma Group and Groupe d'Etude des Lymphomes de l'Adulte Cohort Study. J Clin Oncol 30 (3): 291-9, 2012.
- Anderson RA, Remedios R, Kirkwood AA, et al.: Determinants of ovarian function after response-adapted therapy in patients with advanced Hodgkin's lymphoma (RATHL): a secondary analysis of a randomised phase 3 trial. Lancet Oncol 19 (10): 1328-1337, 2018.
- Weibull CE, Johansson ALV, Eloranta S, et al.: Contemporarily Treated Patients With Hodgkin Lymphoma Have Childbearing Potential in Line With Matched Comparators. J Clin Oncol 36 (26): 2718-2725, 2018.
- Demeestere I, Racape J, Dechene J, et al.: Gonadal Function Recovery in Patients With Advanced Hodgkin Lymphoma Treated With a PET-Adapted Regimen: Prospective Analysis of a Randomized Phase III Trial (AHL2011). J Clin Oncol 39 (29): 3251-3260, 2021.
- Lambertini M, Demeestere I: Another step towards improving oncofertility counselling of young women with Hodgkin's lymphoma. Lancet Oncol 19 (10): 1264-1266, 2018.
- Øvlisen AK, Jakobsen LH, Eloranta S, et al.: Parenthood Rates and Use of Assisted Reproductive Techniques in Younger Hodgkin Lymphoma Survivors: A Danish Population-Based Study. J Clin Oncol 39 (31): 3463-3472, 2021.
- Tarbell NJ, Thompson L, Mauch P: Thoracic irradiation in Hodgkin's disease: disease control and long-term complications. Int J Radiat Oncol Biol Phys 18 (2): 275-81, 1990.
- Hancock SL, Cox RS, McDougall IR: Thyroid diseases after treatment of Hodgkin's disease. N Engl J Med 325 (9): 599-605, 1991.
- Cella L, Conson M, Caterino M, et al.: Thyroid V30 predicts radiation-induced hypothyroidism in patients treated with sequential chemo-radiotherapy for Hodgkin's lymphoma. Int J Radiat Oncol Biol Phys 82 (5): 1802-8, 2012.
- Reinders JG, Heijmen BJ, Olofsen-van Acht MJ, et al.: Ischemic heart disease after mantlefield irradiation for Hodgkin's disease in long-term follow-up. Radiother Oncol 51 (1): 35-42, 1999.
- Hancock SL, Tucker MA, Hoppe RT: Factors affecting late mortality from heart disease after treatment of Hodgkin's disease. JAMA 270 (16): 1949-55, 1993.
- Heidenreich PA, Schnittger I, Strauss HW, et al.: Screening for coronary artery disease after mediastinal irradiation for Hodgkin's disease. J Clin Oncol 25 (1): 43-9, 2007.
- Dabaja B, Cox JD, Buchholz TA: Radiation therapy can still be used safely in combined modality approaches in patients with Hodgkin's lymphoma. J Clin Oncol 25 (1): 3-5, 2007.
- Swerdlow AJ, Higgins CD, Smith P, et al.: Myocardial infarction mortality risk after treatment for Hodgkin disease: a collaborative British cohort study. J Natl Cancer Inst 99 (3): 206-14, 2007.
- van Nimwegen FA, Schaapveld M, Cutter DJ, et al.: Radiation Dose-Response Relationship for Risk of Coronary Heart Disease in Survivors of Hodgkin Lymphoma. J Clin Oncol 34 (3): 235-43, 2016.
- Maraldo MV, Giusti F, Vogelius IR, et al.: Cardiovascular disease after treatment for Hodgkin's lymphoma: an analysis of nine collaborative EORTC-LYSA trials. Lancet Haematol 2 (11): e492-502, 2015.
- Cutter DJ, Ramroth J, Diez P, et al.: Predicted Risks of Cardiovascular Disease Following Chemotherapy and Radiotherapy in the UK NCRI RAPID Trial of Positron Emission Tomography-Directed Therapy for Early-Stage Hodgkin Lymphoma. J Clin Oncol 39 (32): 3591-3601, 2021.
- de Vries S, Haaksma ML, Jóźwiak K, et al.: Development and Validation of Risk Prediction Models for Coronary Heart Disease and Heart Failure After Treatment for Hodgkin Lymphoma. J Clin Oncol 41 (1): 86-95, 2023.
- van Nimwegen FA, Ntentas G, Darby SC, et al.: Risk of heart failure in survivors of Hodgkin lymphoma: effects of cardiac exposure to radiation and anthracyclines. Blood 129 (16): 2257-2265, 2017.
- Galper SL, Yu JB, Mauch PM, et al.: Clinically significant cardiac disease in patients with Hodgkin lymphoma treated with mediastinal irradiation. Blood 117 (2): 412-8, 2011.
- Horning SJ, Adhikari A, Rizk N, et al.: Effect of treatment for Hodgkin's disease on pulmonary function: results of a prospective study. J Clin Oncol 12 (2): 297-305, 1994.
- Martin WG, Ristow KM, Habermann TM, et al.: Bleomycin pulmonary toxicity has a negative impact on the outcome of patients with Hodgkin's lymphoma. J Clin Oncol 23 (30): 7614-20, 2005.
- Prosnitz LR, Lawson JP, Friedlaender GE, et al.: Avascular necrosis of bone in Hodgkin's disease patients treated with combined modality therapy. Cancer 47 (12): 2793-7, 1981.
- Schimpff SC, O'Connell MJ, Greene WH, et al.: Infections in 92 splenectomized patients with Hodgkin's disease. A clinical review. Am J Med 59 (5): 695-701, 1975.
- Behringer K, Goergen H, Müller H, et al.: Cancer-Related Fatigue in Patients With and Survivors of Hodgkin Lymphoma: The Impact on Treatment Outcome and Social Reintegration. J Clin Oncol 34 (36): 4329-4337, 2016.
- Loge JH, Abrahamsen AF, Ekeberg O, et al.: Hodgkin's disease survivors more fatigued than the general population. J Clin Oncol 17 (1): 253-61, 1999.
- Kreissl S, Mueller H, Goergen H, et al.: Cancer-related fatigue in patients with and survivors of Hodgkin's lymphoma: a longitudinal study of the German Hodgkin Study Group. Lancet Oncol 17 (10): 1453-1462, 2016.
- Williams AM, Mirzaei Salehabadi S, Xing M, et al.: Modifiable risk factors for neurocognitive and psychosocial problems after Hodgkin lymphoma. Blood 139 (20): 3073-3086, 2022.
Stage Information for HL
Clinical staging for patients with Hodgkin lymphoma (HL) includes the following:
- Physical examination and history.
- Laboratory studies (including sedimentation rate).
- Thoracic and abdominal/pelvic computerized tomographic (CT) scans with or without positron emission tomography (PET).[
1 ] PET scans combined with CT scans have become the standard imaging for clinical staging.[2 ]
Staging laparotomy is no longer recommended and should be considered only when the results will allow substantially less treatment. Staging laparotomy should not be done in patients who require chemotherapy. If the laparotomy is required for treatment decisions, the risks of potential morbidity should be considered.[
Bone marrow involvement occurs in 5% of patients and is more prevalent in the context of constitutional B symptoms and anemia, leukopenia, or thrombocytopenia. In a retrospective review and meta-analysis of 955 patients in nine studies, fewer than 2% of patients with positive bone marrow biopsy results had only stage I or stage II disease on PET-CT scans.[
Massive mediastinal disease has been defined by the Cotswolds meeting as a thoracic ratio of maximum transverse mass diameter of 33% or more of the internal transverse thoracic diameter measured at the T5/6 intervertebral disc level on chest radiography.[
Staging Subclassification System
Lugano Classification
The American Joint Committee on Cancer (AJCC) has adopted the Lugano classification to evaluate and stage lymphoma.[
| Stage | Stage Description | Illustration |
|---|---|---|
| CSF = cerebrospinal fluid; CT = computed tomography; DLBCL = diffuse large B-cell lymphoma; NHL = non-Hodgkin lymphoma. | ||
| a Hodgkin and Non-Hodgkin Lymphomas. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 937–58. | ||
| b Stage II bulky may be considered either early or advanced stage based on lymphoma histology and prognostic factors. | ||
| c The definition of disease bulk varies according to lymphoma histology. In the Lugano classification, bulk ln Hodgkin lymphoma is defined as a mass greater than one-third of the thoracic diameter on CT of the chest or a mass >10 cm. For NHL, the recommended definitions of bulk vary by lymphoma histology. In follicular lymphoma, 6 cm has been suggested based on the Follicular Lymphoma International Prognostic Index-2 and its validation. In DLBCL, cutoffs ranging from 5 cm to 10 cm have been used, although 10 cm is recommended. | ||
| Limited stage | ||
| I | Involvement of a single lymphatic site (i.e., nodal region, Waldeyer's ring, thymus, or spleen). |  |
| IE | Single extralymphatic site in the absence of nodal involvement (rare in Hodgkin lymphoma). | |
| II | Involvement of two or more lymph node regions on the same side of the diaphragm. | 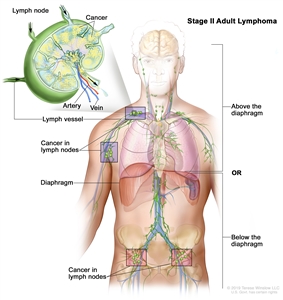 |
| IIE | Contiguous extralymphatic extension from a nodal site with or without involvement of other lymph node regions on the same side of the diaphragm. | 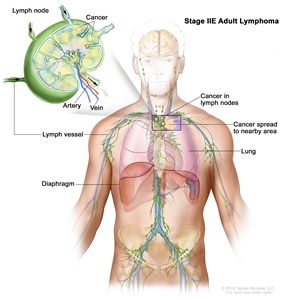 |
| II bulkyb | Stage II with disease bulk.c | |
| Advanced stage | ||
| III | Involvement of lymph node regions on both sides of the diaphragm; nodes above the diaphragm with spleen involvement. | 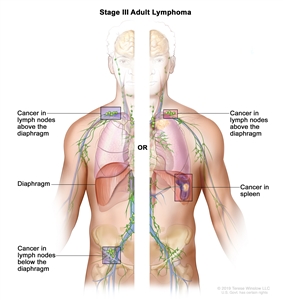 |
| IV | Diffuse or disseminated involvement of one or more extralymphatic organs, with or without associated lymph node involvement; or noncontiguous extralymphatic organ involvement in conjunction with nodal stage II disease; or any extralymphatic organ involvement in nodal stage III disease. Stage IV includes any involvement of the CSF, bone marrow, liver, or multiple lung lesions (other than by direct extension in stage IIE disease). | 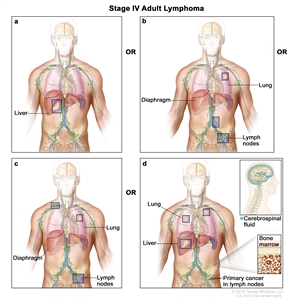 |
| Note: Hodgkin lymphoma uses A or B designation with stage group. A/B is no longer used in NHL. | ||
The E designation is used when well-localized extranodal lymphoid malignancies arise in or extend to tissues beyond, but near, the major lymphatic aggregates. Stage IV refers to disease that is diffusely spread throughout an extranodal site, such as the liver. If pathological proof of involvement of one or more extralymphatic sites has been documented, the symbol for the site of involvement, followed by a plus sign (+), is listed.
| N = nodes | H = liver | L = lung | M = bone marrow |
| S = spleen | P = pleura | O = bone | D = skin |
Prognostic Groups
Many investigators and many new clinical trials employ a clinical staging system that divides patients into three major groups that are also useful for the clinician:[
- Early favorable.
- Early unfavorable.
- Advanced.
The group assignment depends on:
| Whether the patient has early or advanced disease. |
| The type and number of adverse prognostic factors present. |
Early-stage adverse prognostic factors:
- Large mediastinal mass (>33% of the thoracic width on chest x-ray, ≥10 cm on CT scan).
- Extranodal involvement.
- Elevated erythrocyte sedimentation rate (>30 mm/h for B stage [symptoms], >50 mm/h for A stage [symptoms]).
- Involvement of three or more lymph node areas.
- Presence of B symptoms.
Early favorable group: Clinical stage I or II without any of the adverse prognostic factors listed above.
Early unfavorable group: Clinical stage I or II with one or more of the adverse prognostic factors listed above.
Advanced-stage adverse prognostic factors:
For patients with advanced-stage HL, the International Prognostic Factors Project on Advanced Hodgkin's Disease developed the International Prognostic Index with a score that is based on the following seven adverse prognostic factors:[
- Albumin level lower than 40 g/L.
- Hemoglobin level lower than 105 g/L.
- Male sex.
- Age 45 years or older.
- Stage IV disease.
- White blood cell (WBC) count of 15 × 109 /L or higher.
- Absolute lymphocytic count lower than 0.6 × 109 /L or lymphocyte count higher than 8% of the total WBC count.
Advanced group: Clinical stage III or IV with up to three of the adverse risk factors listed above. Patients with advanced disease have a 60% to 80% rate of freedom from progression of disease at 5 years from treatment with first-line chemotherapy.[
References:
- Lister TA, Crowther D, Sutcliffe SB, et al.: Report of a committee convened to discuss the evaluation and staging of patients with Hodgkin's disease: Cotswolds meeting. J Clin Oncol 7 (11): 1630-6, 1989.
- Barrington SF, Kirkwood AA, Franceschetto A, et al.: PET-CT for staging and early response: results from the Response-Adapted Therapy in Advanced Hodgkin Lymphoma study. Blood 127 (12): 1531-8, 2016.
- Urba WJ, Longo DL: Hodgkin's disease. N Engl J Med 326 (10): 678-87, 1992.
- Sombeck MD, Mendenhall NP, Kaude JV, et al.: Correlation of lymphangiography, computed tomography, and laparotomy in the staging of Hodgkin's disease. Int J Radiat Oncol Biol Phys 25 (3): 425-9, 1993.
- Mauch P, Larson D, Osteen R, et al.: Prognostic factors for positive surgical staging in patients with Hodgkin's disease. J Clin Oncol 8 (2): 257-65, 1990.
- Dietrich PY, Henry-Amar M, Cosset JM, et al.: Second primary cancers in patients continuously disease-free from Hodgkin's disease: a protective role for the spleen? Blood 84 (4): 1209-15, 1994.
- Adams HJ, Kwee TC, de Keizer B, et al.: Systematic review and meta-analysis on the diagnostic performance of FDG-PET/CT in detecting bone marrow involvement in newly diagnosed Hodgkin lymphoma: is bone marrow biopsy still necessary? Ann Oncol 25 (5): 921-7, 2014.
- Bradley AJ, Carrington BM, Lawrance JA, et al.: Assessment and significance of mediastinal bulk in Hodgkin's disease: comparison between computed tomography and chest radiography. J Clin Oncol 17 (8): 2493-8, 1999.
- Mauch P, Goodman R, Hellman S: The significance of mediastinal involvement in early stage Hodgkin's disease. Cancer 42 (3): 1039-45, 1978.
- Hodgkin and non-Hodgkin lymphoma. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. Springer; 2017, pp. 937–58.
- Carbone PP, Kaplan HS, Musshoff K, et al.: Report of the Committee on Hodgkin's Disease Staging Classification. Cancer Res 31 (11): 1860-1, 1971.
- Jost LM, Stahel RA; ESMO Guidelines Task Force: ESMO Minimum Clinical Recommendations for diagnosis, treatment and follow-up of Hodgkin's disease. Ann Oncol 16 (Suppl 1): i54-5, 2005.
- Hasenclever D, Diehl V: A prognostic score for advanced Hodgkin's disease. International Prognostic Factors Project on Advanced Hodgkin's Disease. N Engl J Med 339 (21): 1506-14, 1998.
- Rodday AM, Parsons SK, Upshaw JN, et al.: The Advanced-Stage Hodgkin Lymphoma International Prognostic Index: Development and Validation of a Clinical Prediction Model From the HoLISTIC Consortium. J Clin Oncol 41 (11): 2076-2086, 2023.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.